Case Report MemoPart PFO
Patent Forame Ovale Occlusion San Rocco Clinic, Ome, Brescia, Italy Emiliano Boldi, Alberto Lanzone
Background
Patent foramen ovale (PFO) is observed in 25% of the general population; 46% of cryptogenic ischemic strokes are associated with its presence. Diagnostic examinations focusing on PFO are recommended in all patients following a neurological incident before the age of 55. The standard examination performed to detect or exclude PFO is transesophageal echocardiography (TEE) using contrast and the Valsalva maneuver.
Baseline
A Case Report on PFO occlusion in a 65-Year-Old female Patient with indication for percutaneous PFO closure confirmed by cryptogenic stroke episode in the last 3 month. TEE evaluation during the ambulatory visit identified a right-to-left shunt via a simple tunnel, with no aneusysm of the septum primum and no septum secundum hypertrophy.
The PFO procedure was performed in interventional cardiology at Clinica San Rocco in Brescia city, by dr. Emiliano Boldi and Alberto Lanzone.
PFO occluder device MemoPartTM PFO Occluder (Shanghai Shape Memory Alloy Co. Ltd., Beijing, China).
Interventional procedure
The PFO closure was performed as a day-case procedure, under TEE guidance. The procedure was performed from the femoral vein access under local anesthesia. The PFO was crossed with a 5–6 Fr multipurpose catheter and a standard 0.035-inch guidewire from the right atrium. From the inferior vena cava, the Eustachian valve directs the guidewire into the PFO tunnel.
Subsequently, a stiff guidewire is placed in the upper left pulmonary vein to have a better alignment with interatrial septum. A TEE evaluation of the septum primum raising and the size of the consequent left-to-right shunt has been calculated to identify the PFO device size. After that, the long sheath of the Memopart delivery system was pushed beyond the PFO tunnel, the left disc of the device is opened in the left atrium, pulled back to the interatrial spetum and then the right disc is opened in the right atrium and pushed to the PFO entry. Before releasing the device, it was crucial to check the device’s stability with a pull-and-push maneuver (wiggle maneuver) to ensure that the device is well hugged the septum primum and secundum and that there is no interference with the atrioventiruclar valves.
During the percutaneous procedure of PFO closure, TEE is used in combination with fluoroscopy. TEE guidance is needed to cross the PFO, position the closure device, verify if its location is proper, and ensure its stability and efficacy.
Once the stability of the device is confirmed, the occluder is released and both angiographic and bubble tests are performed to detect the presence of a residual shunt. The valsalva maneuver identified a slight residual intraprosthetic shunt that will disappear 3 months after the procedure.
DOWNLOAD PDF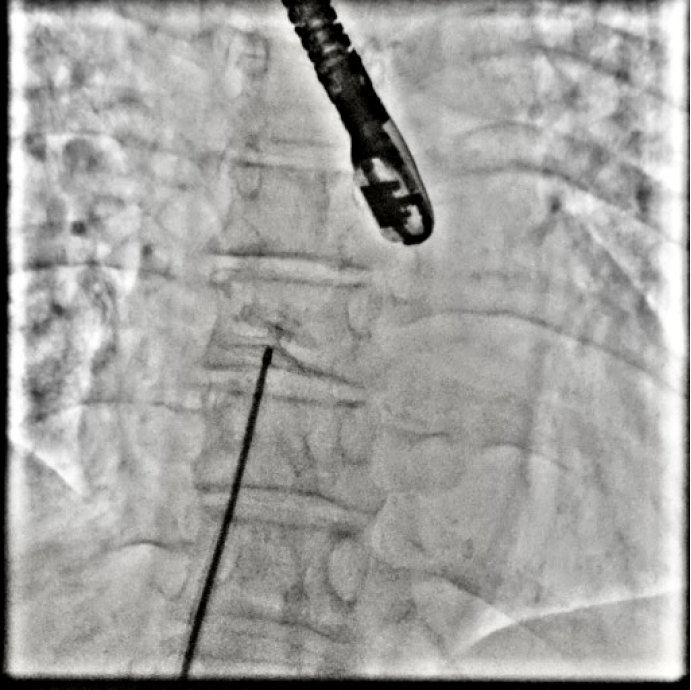
Fig. 1- Deployment of the left and right discs of PFO occluder device MemoPartTM PFO Occluder

Fig. 2- MemoPartTM PFO Occluder is completely released

Fig. 3- Angiographic test are performed to detect the presence of a residual shunt